

Elevating Sterile Manufacturing Impact of the New EU GMP Annex 1

The European Union good manufacturing practice (GMP) guidelines play a vital role in ensuring the quality, safety, and efficacy of medicinal products within the European Union.
One of the key updates to these guidelines is the revised EU GMP Annex 1: Manufacture of Sterile Medicinal Products in 2022 (1). The previous version of Annex 1 was published in 2008, and since then, advancements in technology, quality standards, and regulatory expectations have necessitated an update. Some of the key updates include:
- Enhanced emphasis on quality risk management (QRM) throughout the entire product lifecycle.
- Introduction of a contamination control strategy (CCS) to prevent, detect, and control potential sources of contamination in the manufacturing process.
- Extended scope to a wide range of sterile product types (active substance, excipient, primary packaging material, and finished dosage form) and apply some principles and guidance to other products that are not intended to be sterile.
- More detailed guidance on aseptic processing, including requirements for the design of cleanrooms and associated utilities, environmental monitoring, aseptic process simulation, etc.
- The use of specific technologies such as isolators and closed-system processing.
This article delves into the impact of this regulatory change, its implications, and opportunities for the aseptic manufacturing industry months after Annex 1 came into operation.
Building Patient's Trust
"As patients, we often place our trust in the hands of the pharmaceutical industry and healthcare system to provide us with life-saving medications and products. Good aseptic manufacturing plays a pivotal role in safeguarding our health and well-being," said Hussain Jafri, Executive Director of the World Patients Alliance. The trust in GMP goes beyond aseptic processes and quality control; it assures that medications are manufactured with care and precision. Contaminated drugs can result in severe outcomes such as infections, adverse reactions, and even life-threatening conditions. It is important to understand that the requirement for safe pharmaceuticals is not merely a theoretical idea but a critical matter of life and death for patients.
Ensuring patient safety and drug quality relies on the establishment and adoption of harmonized GMP standards. The assessment and application of these standards require a collaborative effort between drug manufacturers and regulatory authorities.
Annex 1
The new Annex 1 has been a topic of ongoing discussion since its initial draft in 2017, and companies and industry organizations provided comments during the consultation process. However, uncertainties persist, as highlighted at the 2023 PDA Good Aseptic Manufacturing Conference in May. During the conference, approximately 150 attendees were surveyed to identify the most common questions pertaining to Annex 1 that required further clarification and interpretation from authorities (see Figure 1). For example, when surveyed, some asked the following questions on the topics below:
- CCS: Regarding CCS, what is the recommended frequency for effectiveness checks? Which CCS systems have already been reviewed by an inspector, and what were the remarks?
- Low bioburden intermediates: Which principles and guidance in Annex 1 should be applied to low bioburden active substances?
- Pre-use post sterilization integrity test (PUPSIT): Who may conduct a risk assessment as an alternative approach? What process constraints, beyond small volumes, are considered acceptable?
- Restricted access barrier systems or isolators: How can alternative approaches be justified?
- Quality control: What is the required level of "personnel with appropriate training and experience in microbiology"?
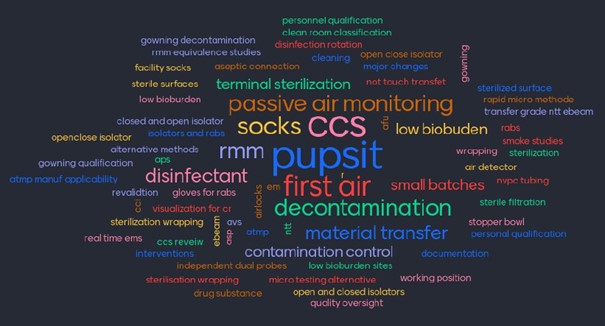 Figure 1 Interactive questionnaire session at the 2023 PDA Good Aseptic Manufacturing Conference in Leipzig,
Germany.
Figure 1 Interactive questionnaire session at the 2023 PDA Good Aseptic Manufacturing Conference in Leipzig,
Germany. The objective of the new Annex 1 was to provide more detailed expectations for manufacturing sterile products, acknowledging that harmonization of standards requires additional specifics. However, the influx of information and details has brought new questions and considerations. The industry has responded by establishing working groups within the industry associations to facilitate discussions, knowledge sharing, and the development of best practices. Various CCS templates and development strategies are available (2), and companies have shared their experiences and proposals through conferences.
Do we manufacture more safe sterile drugs than in the past? Possibly. Drug manufacturers have undertaken Annex 1 gap assessments involving a thorough line-by-line comparison of the requirements outlined in Annex 1 against their current practices. A multidisciplinary team of experts from quality assurance, quality control, production, engineering, maintenance, and supply chain collaborates on this exercise. Identified gaps are prioritized and addressed through remediation efforts, although some corrective and preventive action plans may still be open. To further enhance sterility assurance and minimize contamination risks, implementing a holistic CCS is a crucial step to get the big picture.
Along with this exercise and effort, there is an opportunity to identify process enhancements. An insightful article by McKinsey & Company explores the global sterile manufacturing market, which is anticipated to grow by over 50% by 2028 (3). However, expanding capacity poses challenges regarding installation lead time for new filling lines and a shortage of skilled personnel in sterile manufacturing. To mitigate these challenges, sterile pharma manufacturers can increase capacity without significant capital investments by leveraging operational excellence through digital performance management practices. This includes standardizing and transparently managing key processes, employing analytics, root-cause-driven problem-solving, and automation solutions. Thus, Annex 1 can potentially contribute to boosting capacity to produce more sterile products.
Balance Between Regulation and Principle of Proportionality
Annex 1 emphasizes the application of QRM in the entire document, except where specific limits, frequencies, or ranges are specified. One such example is the specified range for unidirectional airflow systems, which should maintain a homogeneous air speed between 0.36-0.54 m/s at the working position unless there is a scientifically justified reason to deviate from this range. The value of cubic 90 feet per minute, equivalent to 0.45 m/s (±20% results in the required 0.36-0.54 m/s), was established in the early 1960s based on cleanroom development by Willis Whitfield and his colleagues. However, it was never considered as the ideal velocity (4). Annex 1 states alternative approaches "should be supported by a proper rationale, risk assessment, and mitigation." Does this imply that one should adhere to the specified air velocity range without additional justification or conduct a risk assessment? Shouldn't risk management be applied to all measures?
Another ongoing debate pertains to PUPSIT. Sterilizing a drug by filtration is a crucial step, as the filter ensures the final drug's sterility and thus needs to be integral throughout the filtration process. PUPSIT was already required in the previous Annex 1 to check if the sometimes harsh steaming-in-place conditions might have damaged the filter membrane. At the same time, masking effects derived from the product stream could lead to a false positive integrity test result. However, the implementation of PUPSIT for in-place testing introduces additional complexity to the filtration setup, which carries the risk of compromising the sterile boundary downstream of the sterilizing filter.
PDA and BioPhorum conducted thorough scientific investigations on filter masking effects to provide more clarity and support risk assessment approaches. Their findings indicated that such occurrences are very rare, and they developed a method to predict masking effects (5).
Inspectors consistently highlight the importance of PUPSIT as a requirement, with a workaround for "process constraints (e.g., the filtration of very small volumes of solution)." However, it is worth considering that the existing risk is already effectively managed (e.g., no masking potential of the process stream), and the introduction of PUPSIT may potentially introduce new risks. Exploring ICH Q9(R1) Quality Risk Management may offer clarity in this regard, as it provides a framework for addressing key questions related to risk control (6):
- Is the risk above an acceptable level?
- What can be done to reduce or eliminate risks?
- What is the appropriate balance among benefits, risks, and resources?
- Are new risks introduced as a result of the identified risks being controlled?
A regulatory requirement must be suitable and necessary to achieve the desired goal; the associated benefits must be within the principle of proportionality. It is important to note that this is not a plaidoyer against PUPSIT but rather an exploration of other relevant measures to ensure sterility, particularly in situations where PUPSIT may introduce additional risks to the filtration process, and one measure could involve identifying any filter flaw masking effects of the process solution.
Conclusion
The fundamental requirement of GMP, on which all actions and omissions should be based, is to understand the processes, identify potential risks to product quality, develop measures to eliminate or mitigate the risks to an acceptable level, verify the appropriateness of these measures, and consistently apply them with documentation. The revised Annex 1 introduces best practices for aseptic manufacturing and has sparked scientific discussions on guidance details. It is hoped that these discussions will continue and foster collaboration among manufacturers, regulatory authorities, and also suppliers to shape the future of aseptic manufacturing and enhance patient safety and trust worldwide. Hussain Jafri from the World Patients Alliance will address patients' trust in the pharmaceutical industry at the upcoming 2024 PDA Good Aseptic Manufacturing Conference.
References
- European Commission (2022), EU Guidelines for Good Manufacturing Practice Medicinal Products for Human and Veterinary Use, Annex 1, Manufacture of Sterile Medicinal Products
- Parenteral Drug Association (2023), PDA Technical Report No. 90, Contamination Control Strategy Development in Pharmaceutical Manufacturing
- McKinsey&Company (2023), Life Sciences Practices, How sterile pharma manufacturers can grow capacity without capital investment
- David E. Brande Dan C. Milholland Nicholas Haycocks (2017), Why is 90 FPM Considered Standard for Cleanroom Airflow? Pharmaceutical Engineering Vol 37/2
- Brian Thome, Brian Joseph, Dawood Dassu, Jeff Gaerke, Leesa McBurnie, Mandar Dixit, Magnus Stering, Sean Tomlinson, Scott Mills, Stephanie S Ferrante und Carl Weitzmann (2020), Datamining To Determine The Influence Of Fluid Properties On The Integrity Test Values, PDA Journal of Pharmaceutical Science and Technology
- International Conference on Harmonisation (2023). ICH Q9(R1) Quality Risk Management
About the Author
-

Simone Biel, PhD, Merck, Merck
Biel is a Senior Regulatory Consultant at Merck Life Science KGaA Darmstadt, Germany, specializing in single-use technology and filtration in biopharmaceutical manufacturing. Biel provides regulatory guidance to various stakeholders and has assisted numerous drug manufacturers in successfully implementing single-use technology. Beil's primary goal is to ensure product performance aligns with quality and regulatory standards. Beil holds a PhD in microbiology from the University of Frankfurt.